Occipito-Posterior Position
Subject: Midwifery II (Theory)

Overview
This is the most common malposition in which the head initially engages correctly but afterward, the occiput rotates posteriorly rather than anteriorly. 5.2 percent of deliveries are occipito-posterior. The occipito-posterior posture is caused by a weakly bent vertex. The anterior fontanelle (four radiating sutures) is felt anteriorly. The posterior fontanelle (three radiating sutures) may also be felt. It can be caused by a flat sacrum, a weakly flexed head, or weak uterine contractions that do not press the head down into the pelvis with enough force to accomplish proper rotation. An epidural is frequently suggested, and it is critical that the mother receives appropriate fluids.
The most common malposition is occipito-posterior rotation, in which the head initially engages correctly but the occiput rotates posteriorly rather than anteriorly. 5.2 percent of all deliveries are occipito-posterior.
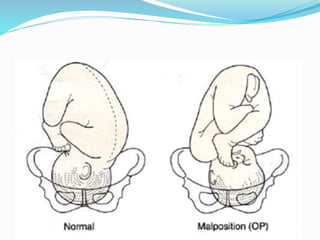
A badly flexed vertex causes the occipito-posterior posture. Anteriorly, the anterior fontanelle (four radiating sutures) is felt. The posterior fontanelle (three radiating sutures) is also palpable. It can be caused by a flat sacrum, a weakly flexed head, or weak uterine contractions that do not press the head down into the pelvis with enough force to accomplish proper rotation.
Management
Due to the fact that occipito-posterior position pregnancies frequently result in protracted labor, intensive maternal and fetal monitoring is essential. An epidural is frequently recommended, and appropriate fluids must be given to the mother.
The mother may feel tempted to push before full dilatation, but this should be avoided. If the head is in a face-to-pubis position, vaginal birth is possible as long as the pelvic size is enough. Otherwise, forceps or a cesarean section might be necessary.
References
-
spinningbabies.com/learn-more/baby-positions/posterior/
- Pathak, Sumita and Sochana Sapkota. A Textbook of Leadership and Management. Bhotahity, Kathmandu: Vidyarthi Pustak Bhandar, 2014
-
nursingcontentbank.blogspot.com/2013/04/occipito-posterior-position.html
- https://www.ncbi.nlm.nih.gov › NCBI › Literature › PubMed Central (PMC)
-
Things to remember title
- This is the most common malposition in which the head engages correctly at first but eventually rotates posteriorly rather than anteriorly.
- 5.2 percent of all deliveries are occipito-posterior.
- A badly flexed vertex causes the occipito-posterior posture.
- Anteriorly, the anterior fontanelle (four radiating sutures) is felt.
- The posterior fontanelle (three radiating sutures) is also palpable.
- It can be caused by a flat sacrum, a weakly flexed head, or weak uterine contractions that do not press the head down into the pelvis with enough force to accomplish proper rotation.
- An epidural is frequently recommended, and appropriate fluids must be given to the mother.
Questions and Answers
Define Occipito-posterior position and how can we manage it ?
Occipito-posterior Position
The head engages correctly at first, but the occiput rotates posteriorly rather than anteriorly in this most typical malposition. Persistent occipito-posterior is seen in 5.2% of births.
A poorly flexed vertex causes the occipito-posterior position. Anteriorly, one can feel the anterior fontanelle (four radiating sutures). The three radiating sutures of the posterior fontanelle may also be palpable.
Management
A protracted labor is frequently the outcome of pregnancies in the occipito-posterior position, therefore close maternal and fetal monitoring is necessary. The woman must have enough fluids, and an epidural is frequently suggested.
It's important to prevent the mother from pushing before she's fully dilated. Vaginal delivery is possible if the head is in a face-to-pubis position and the pelvis is of a reasonable size. Otherwise, a caesarean section or forceps may be necessary.
© 2021 Saralmind. All Rights Reserved.
 Login with google
Login with google